
Successful Adrenalectomy for MEN 2-Related Pheochromocytomas and Medullary Thyroid Cancer
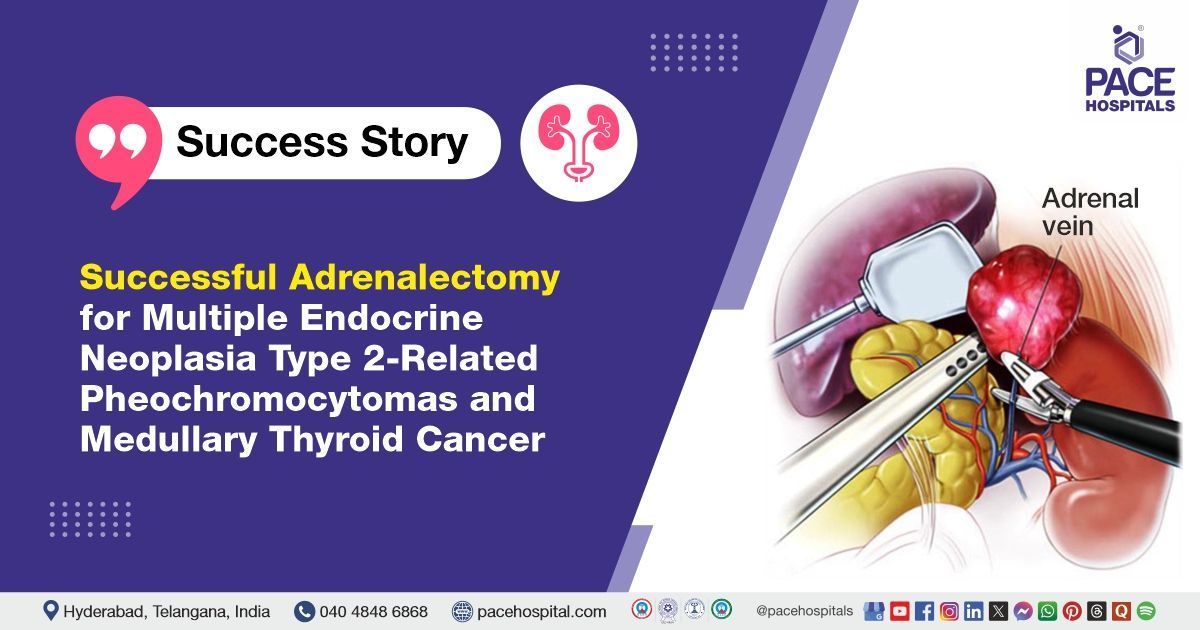
The oncology team along with general surgery team at PACE Hospitals successfully performed a left-sided adrenalectomy under general anaesthesia for a 60-year-old male patient diagnosed with bilateral adrenal pheochromocytomas, as part of Multiple Endocrine Neoplasia Type 2 (MEN2). The procedure was a key step in managing his hormone-secreting tumors and alleviating related complications.
Chief Complaints
A 60-year-old male patient presented to the Endocrinology Department, at
PACE Hospitals, Hitech City, Hyderabad, with complaints of back pain that had been ongoing for the past six months.
History of present illness
The patient was apparently asymptomatic six months ago. He then developed complaints of back pain associated with urinary issues. He was admitted in June 2024 under the Urology team at the hospital.
On evaluation, bilateral adrenal masses were identified, with elevated 24-hour urinary metanephrines and normetanephrines, along with raised plasma-free metanephrines. He was planned for bilateral adrenalectomy and further evaluation for a possible syndromic association; however, he was lost to follow-up. With worsening back pain, he was re-admitted to the hospital.
Past History
The patient is a known case of
type 2 diabetes mellitus and
hypertension, with a history of trauma to the right leg approximately 20 years ago.
General examination
Upon admission to PACE Hospitals, the patient's vital signs were stable. On general examination, notable findings included acanthosis nigricans, a skin condition often associated with insulin resistance or endocrine disorders, and a nodular goiter, which raises concern for potential thyroid involvement. Additionally, the patient exhibited signs of cutaneous lichen amyloidosis and bilateral axillary freckling, suggestive of an underlying genetic syndrome such as neurofibromatosis type 1.
Based on these clinical findings, the medical team decided to initiate a comprehensive endocrine and genetic workup to investigate potential syndromic associations. Further imaging, biochemical evaluations, and genetic testing were planned to confirm the diagnosis and formulate an appropriate multidisciplinary management plan.
Diagnosis
The patient initially presented with clinical features suggestive of an endocrine disorder, including symptoms related to hormonal imbalance. Diagnostic investigations were conducted, which confirmed the presence of bilateral adrenal masses consistent with pheochromocytomas, tumors are known to secrete excess adrenaline and cause symptoms such as high blood pressure, palpitations, and sweating. Given these findings, further evaluation was pursued to investigate possible associated conditions.
A Gallium-68 DOTATATE PET-CT scan was performed, which revealed significant tracer uptake in the thyroid, bones, spine, and bilateral adrenal glands, indicating widespread somatostatin receptor activity. These findings raised suspicion of a systemic neuroendocrine process. In parallel, plasma calcitonin levels were found to be markedly elevated, a biochemical marker suggestive of medullary thyroid carcinoma (MTC)—a rare thyroid cancer originating from parafollicular C-cells.
Due to the patient's complaint of back pain and possible neurological symptoms, a neurological evaluation was conducted. This revealed sign of radiculopathy, prompting an MRI of the spine to assess potential nerve root involvement, which may have been secondary to metastatic disease or compressive lesions.
Based on the combination of pheochromocytomas, elevated plasma calcitonin levels, and thyroid abnormalities, the diagnosis of medullary thyroid carcinoma (MTC) was strongly supported. Given the coexistence of these two endocrine tumors, a diagnosis of Multiple Endocrine Neoplasia Type 2 (MEN2) was established. MEN2 is a hereditary syndrome that includes both pheochromocytoma and MTC and may involve other endocrine glands, necessitating genetic evaluation and family screening.
The patient was ultimately diagnosed with the following conditions:
- Pheochromocytoma – Tumors of the adrenal glands producing excess adrenaline.
- Medullary Thyroid Carcinoma (MTC) – A rare thyroid cancer originating from C-cells.
- Multiple Endocrine Neoplasia Type 2 (MEN2) – A genetic syndrome involving multiple endocrine tumors, including MTC and pheochromocytomas.
These findings indicate the need for a multidisciplinary approach to ensure effective management of the associated conditions.
Medical Decision Making (MDM)
After consulting with the consultant endocrinologist, Dr. Tripti Sharma, along with other consultants Dr. Abhik Debnath, Dr. Sashi Vardhan Janjirala, Dr. Ramesh Parimi, and Dr. Meena K, a comprehensive evaluation was conducted to determine the appropriate course of treatment for the patient.
Their collective expertise led to the conclusion that adrenalectomy under general anaesthesia (GA) would be the most appropriate surgical intervention for the management of the bilateral adrenal masses. This decision was based on a thorough clinical assessment and aimed at ensuring optimal outcomes through timely and definitive treatment.
Surgical procedure
All necessary investigations were completed, and a consultation with an endocrinologist was obtained. The patient subsequently underwent a left-sided adrenalectomy.
This procedure, performed under general anaesthesia, involves the surgical removal of the left adrenal gland, which is responsible for producing vital hormones such as adrenaline, cortisol, and aldosterone. It is commonly indicated in cases of adrenal tumors or pheochromocytomas.
Intraoperative Findings
The operative notes indicate that the patient experienced fluctuating blood pressure and episodes of arrhythmia during the procedure. Once hemodynamic stability was achieved, the patient was positioned in the right lateral decubitus position, and pneumoperitoneum was established using a Veress needle (a small needle (Veress needle) was used to gently fill the abdomen with gas (usually carbon dioxide) to create space for the surgeon to see and operate during the procedure).
Intraoperatively, the left adrenal gland was noted to be enlarged with multiple nodules. A single adrenal vein draining into the renal vein was identified, carefully clamped, and divided. Haemostasis was maintained by controlling smaller arteries using Ligasure and harmonic energy devices. The left adrenalectomy was completed successfully with adequate haemostasis. Due to the patient's borderline performance status, the right-sided adrenalectomy was deferred, and the patient will undergo the right adrenalectomy approximately 1 to 2 months postoperatively.
Postoperative Care
The patient underwent a bilateral adrenal excision under general anaesthesia, following appropriate preoperative optimization with alpha and beta blockers. The postoperative course was initially uneventful.
However, the patient subsequently developed basal atelectasis and a productive cough, which were effectively managed with chest physiotherapy and supplemental oxygen therapy. Additionally, zoledronic acid was administered to alleviate back pain and manage spinal lesions likely related to underlying metastatic involvement or bone fragility.
Discharge Notes
The patient was discharged in a hemodynamically stable condition.
Discharge Medications
Upon discharge, the patient was prescribed a combination of medications, including antibiotics, alpha-blockers, and biguanides for glycaemic control in the management of type 2 diabetes mellitus.
Advice on Discharge
The patient was advised to follow a diabetic-friendly diet along with a low-sodium (low-salt) diet. In addition, chest physiotherapy and regular spirometry exercises were recommended to support respiratory function and enhance pulmonary recovery.
Emergency Care
The patient was informed to contact the Emergency ward at PACE Hospitals in case of any emergency or the development of symptoms like fever, abdominal pain, or vomiting.
Review notes
The patient is scheduled for a follow-up review in one week with the endocrinology, urology, and both medical and surgical oncology teams to ensure coordinated, multidisciplinary care and ongoing evaluation.
Role of Gallium-68 DOTATATE PET-CT in the Evaluation of Bilateral Adrenal Masses and Neuroendocrine Tumours
A Gallium-68 DOTATATE PET-CT scan is a highly sensitive and advanced imaging modality that plays a pivotal role in the detection of bilateral adrenal masses, particularly in cases where neuroendocrine tumors such as pheochromocytomas are suspected. This technique utilizes a radiolabeled tracer that binds specifically to somatostatin receptors, which are frequently overexpressed in neuroendocrine tumors.
The scan generates high-resolution, whole-body images that accurately delineate the location, size, metabolic activity, and extent of tumor involvement. It is especially useful in identifying lesions in the thyroid, adrenal glands, bones, and spine, providing crucial information for comprehensive disease assessment. The modality also excels in distinguishing benign from malignant masses, assessing bilaterality, and detecting extra-adrenal spread or associated neoplasms.
This makes Gallium-68 DOTATATE PET-CT an essential tool in the staging, treatment planning, and monitoring of adrenal tumors, particularly in hereditary syndromes like Multiple Endocrine Neoplasia Type 2 (MEN2). Its precision supports personalized care and enhances long-term disease management.

Share on
Request an appointment
Fill in the appointment form or call us instantly to book a confirmed appointment with our super specialist at 04048486868
Appointment request - health articles


Our Locations – Find the Best Hospital Near You
Metro Pillar Number C1772, Beside Avasa Hotel, Hitech City Road, Near HITEC City Metro Station, Hyderabad, Telangana, India.
Mythri Nagar, Beside South India Shopping Mall, Hafeezpet, Madeenaguda, Hyderabad, Telangana, India.
040 4848 6868
Payment in advance for treatment at PACE Hospitals, Hyderabad, Telangana, India (Pay in INR ₹)
For Bank Transfer:-
- Bank Name: HDFC
Company Name: Pace Hospitals
A/c No.50200028705218
IFSC Code: HDFC0000545 - Bank Name: STATE BANK OF INDIA
Company Name: Pace Hospitals
A/c No.62206858997
IFSC Code: SBIN0020299
Scan QR Code by Any Payment App (GPay, Paytm, Phonepe, BHIM, Bank Apps, Amazon, Airtel, Truecaller, Idea, Whatsapp etc).

CONTACT US
Call: +914048486868
WhatsApp: +918977889778
Email: info@pacehospitals.in
FOLLOW US
SUBSCRIBE
Subscribe to our newsletter and stay updated with the latest health information.
ABOUT US
QUICK LINKS
Disclaimer
General information on healthcare issues is made available by PACE Hospitals through this website (www.pacehospital.com), as well as its other websites and branded social media pages. The text, videos, illustrations, photographs, quoted information, and other materials found on these websites (here by collectively referred to as "Content") are offered for informational purposes only and is neither exhaustive nor complete. Prior to forming a decision in regard to your health, consult your doctor or any another healthcare professional. PACE Hospitals does not have an obligation to update or modify the "Content" or to explain or resolve any inconsistencies therein.
The "Content" from the website of PACE Hospitals or from its branded social media pages might include any adult explicit "Content" which is deemed exclusively medical or health-related and not otherwise. Publishing material or making references to specific sources, such as to any particular therapies, goods, drugs, practises, doctors, nurses, other healthcare professionals, diagnoses or procedures is done purely for informational purposes and does not reflect any endorsement by PACE Hospitals – your trusted hospital near me.

